

This post is a continuation on my discussion about Patient Health Literacy. The narrative that resulted from this study has been published on Amazon. See my Memoir page. The original source that I used for my study can be found at https://bcbecky.com.
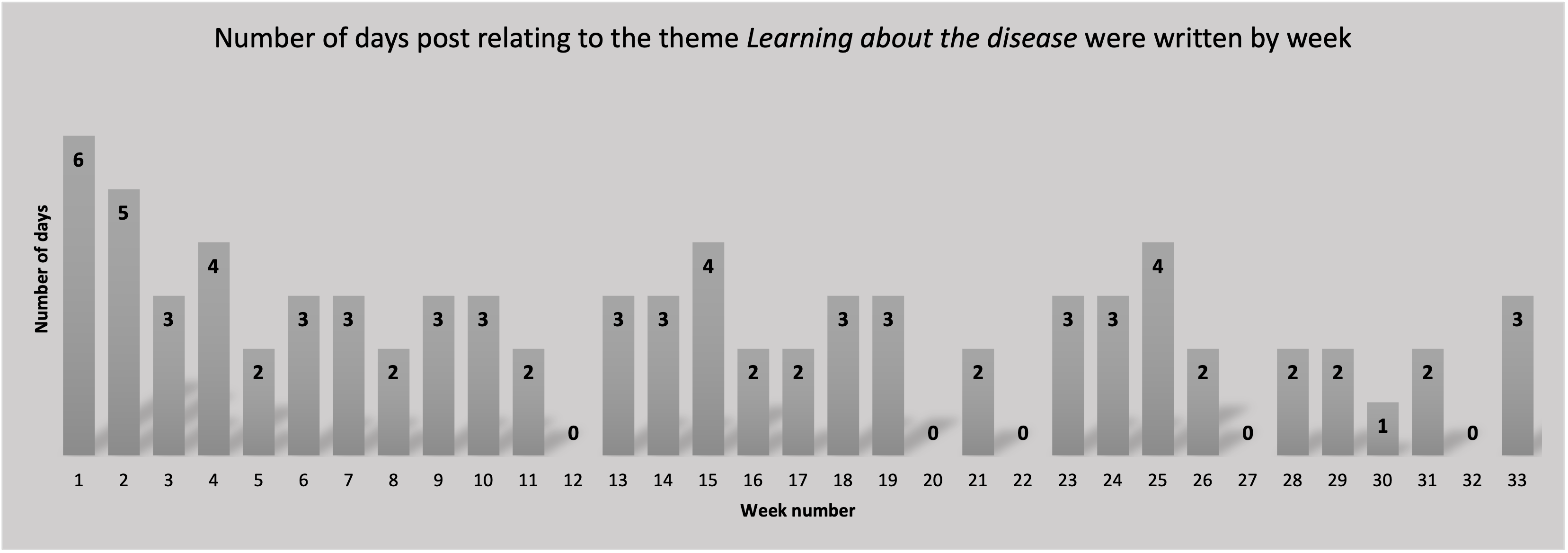
From among the 237 blog posts, I coded 92/237 (38.8%) with the category, Learning about the disease. The distribution of number of days per week that I wrote one or more posts that were coded as Learning about the disease, Figure 4, shows interactions almost every week. This is particularly interesting because it shows that the learning did not just happen at diagnosis, rather I continued to learn and share my learnings throughout the study period.
In reviewing the posts categorized as Learning about the disease, I constructed the following themes: (1) sourcing experts, (2) sourcing the Internet, (3) sourcing academic articles, and (4) sourcing peers. The theme sourcing experts applies to posts where I echo the information I receive from healthcare providers. The theme sourcing the Internet applies to posts where I include information from trusted Internet sources. The theme sourcing academic articles applies to posts where I include references to academic literature. The theme sourcing peers applies to posts where I describe information that I have gathered from peers such as through support group meetings. Peer sources includes blog posts of other cancer survivors. I discussion each of these themes in more detail in the in the following sections.
Sourcing experts
When I was initially diagnosed, I knew very little about breast cancer. In my early posts I would parrot back of the words I heard from my healthcare providers. For example, in It all started… (June 14, 2014) I say, “I’ve been told that the majority of women who get breast cancer do not have relatives with cancer”. As I gather more specific information, I include my interpretation and feelings associated with the information I’m receiving. For example, in Double-Mastectomy and chemo (June 19, 2014), I write not just about the disease characteristics, but also what those characteristics mean and how that translates into a treatment plan. At this point, I am echoing the information the I received from an oncologist. I’m not referencing any other source. More importantly, in this post I’m not just talking about the data itself (that is the pathology), I’m also talking about what that data means and how that information affects the recommended treatment options.
Sourcing the Internet
Within support groups, I often heard the women say to someone who is newly diagnosed ‘do not look at the Internet’. And yet, it was the Internet that I went to when I needed to look up medical terminology. When interpreting my pathology report, I tell readers of my blog that if they want more information on how to understand pathology reports, to look at http://breastcander.org. I refer to this site several times within the blog, as it provided useful information regarding breast cancer and treatment options.
When I wanted a description of medical terms, or when I wanted to validate something that I heard from either support groups or healthcare providers, I went to trusted sites on the Internet. In Significance of dates and getting ready for chemo (June 26, 2014), I write about my reflections on the chemotherapy preparation class that my husband and I attended. I share a couple of resources: a book that I found to be not very useful; and, a website, http://chemocare.com, that was very useful. I find it particularly interesting that advice is often given to ‘not look at the internet’, and yet the better and more current resources shared are those found on websites rather than books, which quickly become outdated.
Sourcing academic articles
Initially, I was unable to read academic sources, rather, I relied on my husband to do that research. However, when I had to make a decision regarding surgery, I reached into the academic literature to do an analysis on what the surgery and the expected results of neoadjuvant chemotherapy. For example, in Breast reconstruction – academic analysis (September 22, 2014), I write about the knowledge I gained through reading academic articles relating to the type of breast reconstruction surgery I was debating. In addition to sharing some of the key findings from the academic articles, I also shared terminology definitions such as “Autologous reconstruction is reconstruction that involves the patient’s own tissue (e.g. DIEP flap, TRAM flap).” In Pathological Complete Response (September 23, 2014), I write about the knowledge I gained, and my interpretation of academic articles associated with the expected outcomes of neo-adjuvant chemotherapy. I not only provide key findings, but I provide my commentary on the findings. I’m sharing both the findings from the articles and my interpretation of that information and how it applies to my situation.
Sourcing peers
In addition to healthcare providers, friends connected me to a fellow breast cancer survivor. I see echoes of conversations I had with here in my blog, for example when I say “choose who you want to trust, and then trust them” (A long day, June 19, 2014). By the time I was to start treatment, I was familiar with some of the expectations around treatment. For example, in This too shall pass (July 16, 2014), I say that “during support group last Saturday, one of the ladies explained what the Neulasta bone point felt like. I had been warned.”
Perhaps the biggest benefit from support groups was the normalization of medical terminology and the generic breast cancer treatment process. Specifically, in A photo shoot and getting ready for surgery (November 18, 2014), I write about the process of the surgery. I specifically talk about the “injection of some nuclear isotope into each breast that helps to identify the sentinel node, and the insertion of wires to guide the surgeon to the exact location of each of the tumors”. By the time I wrote about the procedure, the concepts had been ‘normalized’ for me. I had heard about it so many times at support group that I came to think of the process as ‘normal’. It was just something that I needed to do. Further, in Breast reconstruction – Academic analysis (September 22, 2014), I point to another blogger’s post before I refer to the academic literature: “First off, I should start by pointing out an important blog post written by Nancy Stordahl on why breast reconstruction is not a boob job (2013). When looking at patient satisfaction, I focused on post-cancer reconstruction which is a lot more complex than cosmetic reconstruction.”
I don’t share a lot of the medical information that I received in support group. In part because I often validated this information with my healthcare provider and then reported it in my blog as being from my healthcare provider. In Flyin’ (November 26, 2014), I write about information that I learned from various support groups pertaining to lymphedema, and then how I looked into the academic research about it, sharing some key points from the research. Here I am showing how the information I received through support group helps me know what to look up, but also how I do not directly trust the information in support group, rather I look to more trustworthy sources.
Summary
In order for patients to be partners with their healthcare team in making appropriate decisions, patients need disease-specific information (Wallberg et al., 2000). When I was diagnosed, I knew almost nothing about breast cancer. I needed to use multiple sources in order to learn about the disease. My analysis of the category Learning about the disease shows that I continued to learn about the disease throughout the treatment process. Under the category of Learning about the disease, I constructed the following four themes (1) sourcing experts, (2) sourcing the Internet, (3) sourcing academic articles, and (4) sourcing peers. Within these information sources, I did not only share the information directly, I also shared the way in which I was interpreting the information. In addition, as time progressed, I increased where I received my information, using multiple sources to validate what I was learning.
I began my learning about breast cancer through information I received directly from expert sources, that is my healthcare providers. When I needed clarification on terminology or more detailed medical information, I sought out trusted Internet sources. When I was ready to read academic literature, I searched the literature for information that would help me make treatment decisions. The different information and advice sources sometimes overlapped, where at other times they didn’t. I had to learn how to discern not only where I could get information, but also what types of information I could get from where, and how reliable that information was. There were so many nuances to information that I didn’t always appreciate at the time, and some that I still don’t appreciate. Throughout the process I negotiated the information that I received from expert sources, Internet sources, and academic sources. Although I gathered information from peer sources, I did not directly trust that information, rather I used trusted sources to validate what I had learned through peer sources. Patients experiencing critical or chronic illness have a need to learn appropriate sources for different types of information to help them learn about the disease and what it means to live with the disease.
Where do you find your health information? What sources do you find reliable? Where do you learn about how to live with the disease?
Leave a Reply